A mole on the back and a mole on the cheek are anatomically the same thing, a cluster of melanocytes at or below the dermo-epidermal junction. From the perspective of skin-cancer risk they are identical, and a consultant will assess them with the same dermatoscopy and the same ABCDE framework. From the perspective of removal, they are very different procedures.
Facial moles are removed differently because the face is not uniform skin. Each region (forehead, cheek, nose, periorbital, lip, chin) has its own thickness, its own tension lines, its own scar behaviour, and its own anatomical structures sitting just beneath the surface. A technique that gives a clean linear scar on the back can leave a visible step, a pulled eyelid, or a distorted lip on the face, depending exactly where it is performed.
This guide walks through what makes the face surgically distinctive, why every region has its own approach, and how a consultant plastic surgeon plans a removal so the scar settles into the skin's natural lines rather than across them. Written by a consultant who specialises in facial surgery and performs hundreds of these procedures each year.
Why the face needs its own approach
Three things distinguish facial mole surgery from body surgery, and each shapes how a consultant plans the procedure. First, visibility: the face is the part of the body other people see. A scar 6 mm long on the back is hidden by clothing; the same scar on the cheek is in every photograph and every conversation. The cosmetic threshold is unforgiving. Second, anatomy: the face has densely packed structures (facial nerve branches, blood vessels, the parotid duct, lacrimal apparatus) sitting just below skin. A poorly planned excision can damage any of them. Third, tissue characteristics: facial skin varies from millimetre-thin (eyelid) to thick and sebaceous (nose), and each behaves differently under tension and during healing.
The combined effect is that facial mole removal is its own discipline within plastic surgery and dermatology. The same surgeon who removes a back mole in 15 minutes may take 45 minutes for a similar lesion on the alar rim of the nose. The extra time is not bureaucratic; it is consciously buying a better cosmetic and functional result.
What follows is a tour of the six facial zones we treat most often, with the considerations specific to each. The intention is to give you a useful mental model of why the consultant might recommend a particular technique, how long the procedure will take, and what the likely scar will look like.
Relaxed skin tension lines: the most important map
The single most important concept in facial scar planning is the orientation of relaxed skin tension lines (RSTLs), often credited to the surgeon Albert Borges who described them in detail in the 1970s.[1] These are the natural creases the skin falls into at rest, perpendicular to the underlying muscles' direction of pull. Lines that run with them heal cleaner, fade further, and become almost invisible over time. Lines that cut across them widen, raise, and remain visible for years.
Practically, the consultant marks the RSTLs with a fine surgical pen before any incision. On the forehead they run horizontally, on the cheek they run obliquely from the eye toward the corner of the mouth, on the nose they run vertically across the bridge but switch direction near the alar rim, and on the chin and jaw they are largely vertical. The marked lines determine the orientation of the elliptical excision, because the long axis of the ellipse must align with the RSTL for the scar to fall into the line.
This is the reason cosmetic facial scars on a well-planned excision often fade to near-invisibility, and the reason poorly planned excisions remain visible for life. The technique is taught in every plastic surgery training programme; it is also the difference between a routine general-practice excision and a consultant plastic-surgery excision. For face moles, this matters.
Forehead and temple
The forehead is one of the more forgiving facial sites. Skin is moderately thick, RSTLs are uniformly horizontal, and underlying tissue is generous, which gives a consultant predictable closure with low tension on the wound.
The two considerations that shape technique here are brow position and hairline. An excision close to the brow needs careful planning to avoid lifting it asymmetrically; a few millimetres of vertical pull on a sutured wound can leave one brow visibly higher than the other for months. An excision close to the hairline often runs along it deliberately, hiding the resulting scar in the natural transition zone.
Expected outcome for forehead excisions: a thin horizontal scar that fades to faint pink by month three and to near-invisible by month nine. Patients should expect daily SPF 50+ on the area for the full first year, plus silicone gel for three to six months. The forehead heals well; minor adjustments are rare.
Cheek
The cheek covers a large area with regionally variable RSTL direction. The lateral cheek (closer to the ear) tends to follow oblique lines from the eye to the corner of the mouth; the medial cheek (closer to the nose) shifts direction as it approaches the nasolabial fold.
For small benign moles (<6 mm), shave excision often gives the best aesthetic result, leaving a flat pale circle that fades over months. For larger moles or any lesion needing definitive histology, full-thickness elliptical excision aligned to the local RSTL is the standard. For lesions over 1 cm or in cosmetically sensitive locations, the consultant may use a small skin flap (a borrowed piece of nearby skin rotated into the defect) to redistribute the tension and avoid pulling on adjacent structures.
The cheek's main risk is lid distortion if the excision is high enough to communicate tension upward to the lower eyelid. A skilled consultant either avoids this geometry or uses a flap to break the tension vector. This is one of the situations where the choice of surgeon and technique matters most.
Nose
The nose is one of the harder facial sites for mole removal, for two reasons. First, the skin is thick, sebaceous and pinned tightly to the underlying cartilage, particularly on the lower third (the tip and alar rims). This limits how much skin can be 'borrowed' from neighbouring tissue to close the wound. Second, the nose is surgically central to the face; any distortion is immediately visible.
For small benign nasal moles, shave excision is often the best option, especially on the dorsum (bridge) where the resulting flat scar fades well. For full-thickness excision, the surgical strategy depends on size and exact location: the upper third of the nose tolerates simple closure reasonably well, the lower third often requires a local flap (bilobed or rotation) to redistribute tissue without distorting the alar rim or the columella.
Patients considering nose mole removal should expect a longer consultation discussion about technique options. The consultant will often recommend dermatoscopic confirmation of benign features before any cosmetic-only removal, because nasal moles in older adults can sometimes be early basal cell carcinomas that look mole-like at a glance and need different surgical margins.
Periorbital, around the eye
The skin around the eyes is the thinnest on the body and arguably the highest-stakes territory for facial mole surgery. A poorly planned excision on the lower lid can pull the lid downward (ectropion) or distort tear-film drainage, both of which are visible and functionally problematic.
Periorbital mole excisions are best performed by a consultant plastic surgeon with specific experience in eyelid surgery. The surgical plan often involves a Z-plasty or a flap rather than a simple ellipse, to redistribute tension along multiple axes and avoid any vertical pull on the lid margin. The procedure itself is sometimes longer than 60 minutes for a lesion that would take 15 minutes elsewhere on the face.
Cosmetically, the periorbital region is forgiving in a different way. The thin skin tends to heal with minimal hypertrophy and scars fade well over six to nine months, often blending into the existing fine wrinkles around the eye. The risk to manage is functional rather than aesthetic: protect the lid margin, the lacrimal apparatus, and the levator muscle that lifts the upper lid.
Lip and vermilion border
The lip is the most demanding facial zone for mole surgery. The vermilion border, the precise transition between the red lip and the surrounding skin, is one of the most visible anatomical landmarks on the face, and any mismatch of even half a millimetre after suturing creates a permanent visible step.
The standard technique for a mole on or near the vermilion border begins with the surgeon marking the border on each side of the planned excision in surgical ink before any incision is made. The marks act as alignment points during closure. The tissue is closed in layers (mucosa, muscle, vermilion, skin) so each layer aligns precisely. A general-practice 'oval ellipse and stitch' approach is not sufficient here.
Expected outcome: with a consultant-plastic-surgery technique, the resulting scar usually settles to a thin pale line that mostly disappears into the lip's natural texture by month nine to twelve. With a poorly planned closure, the scar can leave a permanent step or notch. This is the zone where the choice of surgeon makes the largest difference to the final result.
Chin and jawline
The chin and jawline are the more forgiving facial zones, with vertical to slightly oblique RSTLs and reasonably elastic skin. Excisions placed along the natural lines heal cleanly, and most leave a thin linear scar that becomes barely visible from a normal conversational distance by month six.
Two considerations shape technique. First, beard-bearing skin in many men contains hair follicles that can sometimes spit out small inclusion cysts during healing, briefly inflamed before resolving. This is normal and self-limiting. Second, the angle of the jaw runs over the parotid gland, and any excision deeper than the dermis at this site needs awareness of the marginal mandibular branch of the facial nerve, which is why we do not recommend deep excisions in this zone outside a consultant plastic-surgical setting.
Cosmetic outcome on the chin and jawline is typically very good. Patients are often surprised at how well a chin scar fades, particularly compared to the mental picture they had before booking. SPF and silicone are the same protocol as everywhere else: 12 months of daily SPF 50+, three to six months of silicone gel.
What to do before booking a facial mole removal
Three steps make the consultation more useful. First, identify exactly which mole or moles you want addressed, take dated phone photographs from a few angles, and have a clear sense of how much they bother you. The more specific you are, the more usefully the consultant can plan.
Second, ask explicitly about histology. Even a 'cosmetic' facial mole that looks benign on dermatoscopy should be sent for pathology, because the cost of missing an unexpected early melanoma in facial skin is meaningful. Any clinic that offers laser mole removal on the face should be approached with caution; the diagnostic-evidence argument we make against laser everywhere on the body applies double on the face, where unexpected histology surprises are clinically significant.
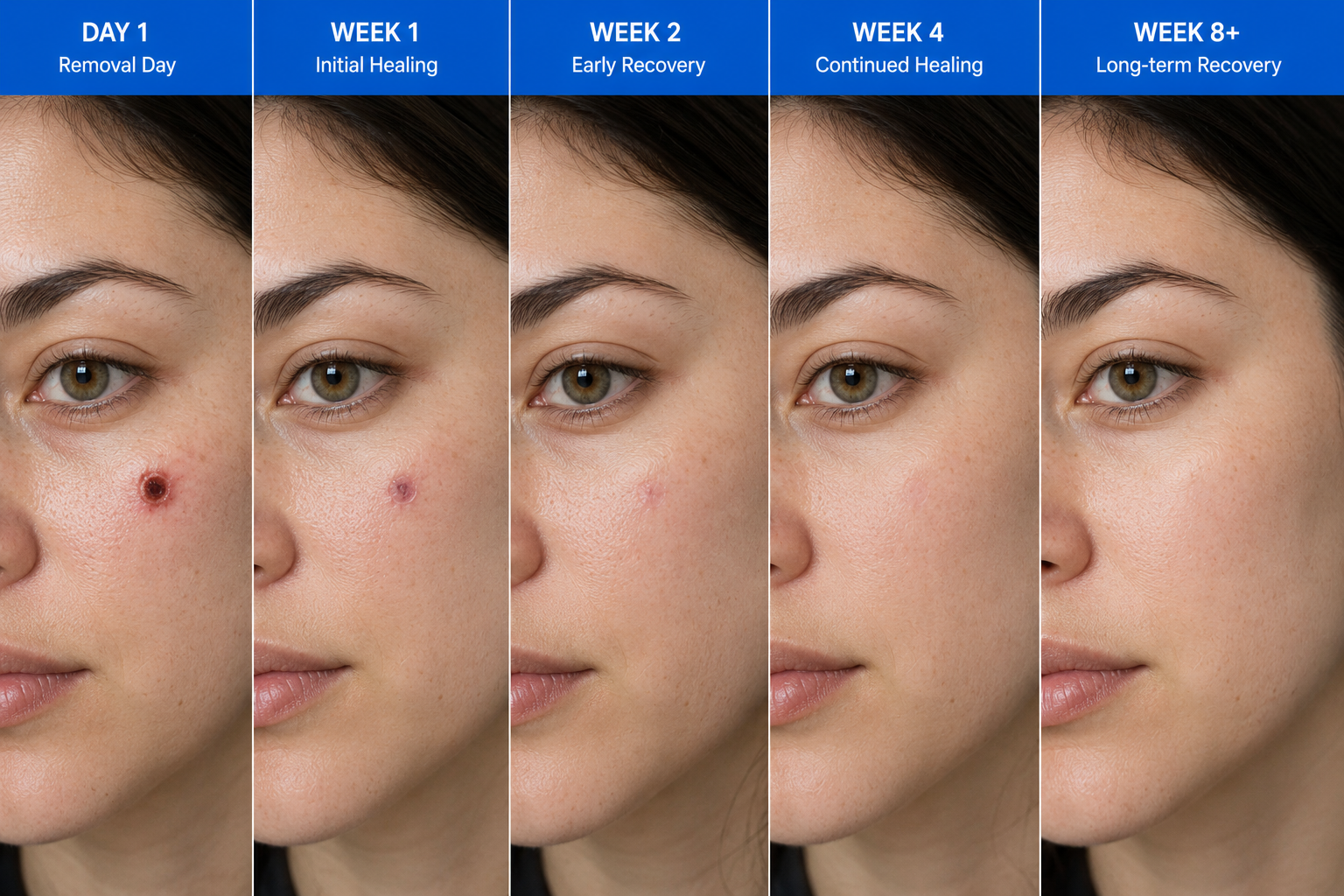
Third, set realistic expectations on scar timeline. A facial scar at six weeks looks different to the same scar at nine months. The trajectory is consistently better than patients expect, but the journey takes a year. Plan major events (a wedding photograph, a video shoot) at least four to six months after the procedure, and longer if the lesion is on the lip or eyelid where remodelling takes the longest.
Common questions
Frequently asked
References
Sources cited
- Borges AF. Relaxed skin tension lines (RSTL) versus other skin lines. Plast Reconstr Surg. 1984;73(1):144-150. View source
- Lee KK, Mehrany K, Swanson NA. Surgical revision of cutaneous scars. Dermatol Clin. 2005;23(1):141-150. View source
- Wong VW, Sorkin M, Glotzbach JP, Longaker MT, Gurtner GC. Surgical approaches to create murine models of human wound healing. J Biomed Biotechnol. 2011;2011:969618. View source
- Sherris DA, Larrabee WF Jr, Murakami CS. Management of scar contractures, hypertrophic scars, and keloids. Otolaryngol Clin North Am. 1995;28(5):1057-1068.
- British Association of Dermatologists. Skin surgery information for patients. View source