Sun protection is one of those topics where everyone has heard the headline, SPF 30, reapply often, and almost no-one applies it correctly. The result is millions of UK adults using sunscreen the way they were taught at school, half-protected, and accumulating UV damage they intended to prevent.
The good news is that getting this right is not complicated. There are five things to understand, three habits that move the dial, and one number on a bottle that matters more than the SPF. Spend ten minutes with this guide and you will protect your skin more effectively than 90% of UK adults, including most who think they're already doing it.
Written and medically reviewed by a GMC-registered consultant dermatologist who sees the consequences of UV damage daily. Not preachy. Not perfectionist. Just the small set of decisions that genuinely change melanoma and ageing risk for adults living in the UK.
What UVA and UVB actually do
Sunlight reaching the UK ground contains two types of ultraviolet radiation that affect skin: UVB and UVA. They behave differently and matter for different reasons.
UVB is the higher-energy, shorter-wavelength part of the spectrum. It is mostly absorbed in the upper layers of the skin (the epidermis), and its main effect is acute, it burns. UVB is the dominant driver of sunburn, of squamous cell carcinoma, and a significant contributor to melanoma. It is most intense between 11am and 3pm in summer in the UK, and it is largely blocked by ordinary glass.
UVA is lower-energy, longer-wavelength radiation. It penetrates much deeper into the skin (into the dermis), and its main effects are chronic: photoageing (fine lines, pigmentation, loss of elasticity) and a meaningful contribution to melanoma development.[1] UVA is present at almost the same intensity year-round, throughout daylight hours, and passes through ordinary window glass. This is why sun damage accumulates in office workers and drivers who don't think they are getting much sun.
Effective protection has to cover both. A sunscreen that protects only against UVB will let UVA through to do its slower damage. The label to look for is broad spectrum, plus a UVA rating: in the UK, look for a 4 or 5 star UVA rating on the bottle, or the European 'UVA' in a circle, which guarantees the UVA protection is at least one third of the SPF figure.
What SPF actually means
SPF stands for Sun Protection Factor. It is a UVB-specific measure: roughly, the multiplier on how long it would take you to burn compared to bare skin under standardised conditions. SPF 30 lets through about 1/30th of the UVB; SPF 50 lets through about 1/50th.
In percentage terms: SPF 15 blocks about 93% of UVB. SPF 30 blocks 97%. SPF 50 blocks 98%. SPF 100 blocks 99%. The marginal benefit above SPF 50 is small, which is why no UK regulator labels anything above SPF 50+. The big jump is from no sunscreen to SPF 30; the smaller jump is from SPF 30 to SPF 50; and almost nothing useful happens above that.
What SPF is not is a measure of how long you can stay in the sun. The 'multiplier' framing is technically accurate under laboratory conditions, but in real life it falls apart because you are not applying the right amount, you are sweating, and you are towelling. So the right way to think of SPF is as a margin of safety, not a license to extend exposure. SPF 30 daily, applied correctly, is genuinely effective. SPF 100 applied half-heartedly is worse than SPF 30 applied properly.
Application: the part most people get wrong
The single most common mistake in real-world sunscreen use is applying too little. The SPF figure on the bottle is measured at 2 milligrams of cream per square centimetre of skin (2 mg/cm²). Studies repeatedly show that the average adult applies between a quarter and a half of that, which means an SPF 50 cream behaves more like SPF 12 to 25 in practice.[2]
The practical heuristics. For full body in summer wear, an adult needs about 30 to 35 ml of cream, roughly a shot-glass full. For face, neck and ears, two finger-lengths of cream squeezed onto two fingers. For each arm, two finger-lengths. For each leg, three finger-lengths. For the torso, front and back, four finger-lengths each. If your sunscreen feels too generous, you're probably applying it correctly for the first time.
The other half of the application story is timing. Apply 15 to 20 minutes before sun exposure, not at the beach. This gives the cream time to bind to the stratum corneum (the outer skin layer) and form an even film. Applying after you're already out tends to leave streaks and undersaturated areas, particularly on hairy skin and at junctions like the hairline and behind the ears.
Reapplication: every two hours, and immediately after
Sunscreen is not a one-application product. Sweat, towelling, water and skin shedding all degrade the protective film over the course of a few hours. The standard UK recommendation, every two hours plus immediately after swimming or heavy sweating, is supported by the regulatory testing standards and is the right rule for any sustained outdoor exposure.[3]
Practical implementation matters more than the rule. Carry a small bottle in your bag for top-ups; keep one in the car for school runs and dog walks; pack one with your swimming kit. The friction between knowing the rule and actually doing it is what most patients fail on, not the rule itself.
Two myths worth dispelling. 'Water-resistant' sunscreens are tested at 40 or 80 minutes of immersion, not all-day. Even the 80-minute formulations need reapplying after swimming, both because the rating is conservative and because towelling removes more than the water itself does. And 'spray' sunscreens are convenient but tend to be applied at half the dose of cream, particularly in windy outdoor conditions; if you use spray, double the application time and rub it in.
The UK-specific context
Two things shape sun protection differently in the UK than in sunnier countries. First, the UV index is genuinely lower for most of the year. Outside June, July and August, UVB intensity is rarely high enough to cause acute burning in normal weather. This is why daily SPF 30 is sufficient for most of the year and SPF 50 is the summer/holiday standard rather than the year-round one.
Second, UV intensity in the UK varies enormously between cloud cover, latitude (northern Scotland is meaningfully different from southern England), and altitude. The Met Office publishes a daily UV index that's a good guide; UV index 3 to 5 is moderate, the threshold at which most pale-skinned adults will burn within an hour of unprotected midday exposure. Index 6+ is high, treat it like a sunny holiday.
Vitamin D is worth one paragraph. The UK winter sun is too weak to produce much vitamin D between October and March even with sun exposure, which is why the NHS recommends a daily 10 microgram supplement for everyone in those months.[4] In the summer months, brief incidental exposure (15 to 20 minutes of forearms and face, a few times a week) provides plenty of vitamin D without meaningful melanoma risk. Sun protection does not deplete your vitamin D in any clinically significant way; supplement in winter and protect properly in summer.
Habits that beat any sunscreen
Sunscreen is the last line of defence. Three habits, used together, dramatically reduce UV exposure before any cream is applied, and they cost less and last longer than any tube on a shelf.
Shade. Avoid the strongest sun (11am to 3pm in UK summer). A pre-booked lunch reservation under a parasol is more effective than reapplying SPF on the beach. Hats. A wide-brimmed hat (4 inches or wider) shades the face, ears and neck, the highest-risk facial sites for skin cancer. Baseball caps don't shade the ears or neck, which is why hat-wearing patients still get sunburn on the upper helix and neck. Clothing. Tightly woven fabric is a remarkably effective UV barrier; UPF-rated rash vests for swimming and outdoor sport reduce exposure to a fraction of what bare skin would receive. The British Association of Dermatologists endorses this as the cornerstone of a sun-protection plan, with sunscreen as the supplement, not the substitute.[5]
Sunglasses matter too. The skin around the eyes is some of the thinnest on the body and one of the highest-incidence sites for basal cell carcinoma. Wraparound sunglasses with full UVA and UVB protection (a CE or BS EN ISO 12312-1 mark) protect both the eye itself and the periorbital skin. Cheap fashion sunglasses without UV ratings can be worse than no sunglasses, because they dilate the pupil under reduced visible light while letting UV through.
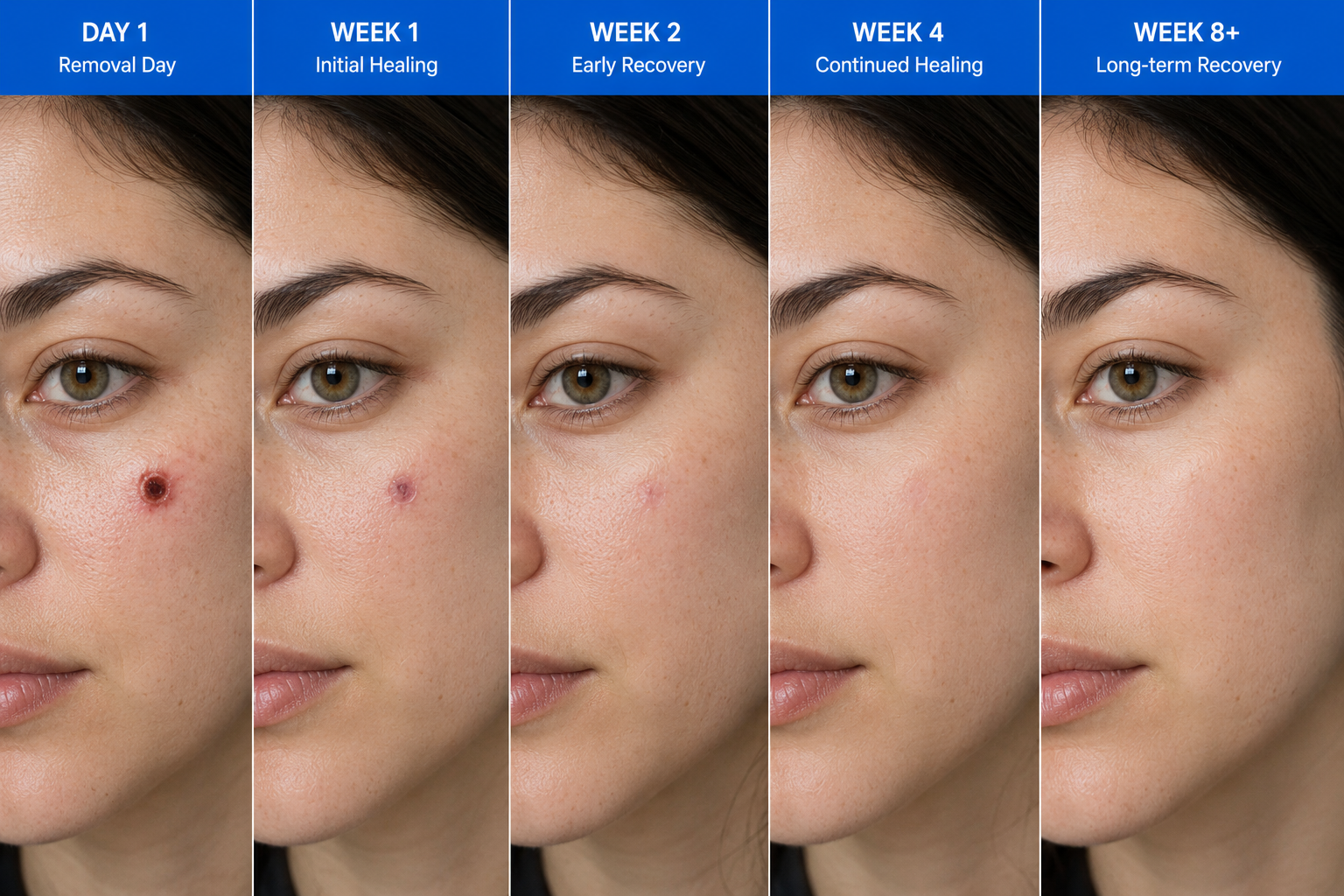
Sun protection after mole removal or biopsy
If you've had a mole removed, the surgical site needs more aggressive sun protection than the surrounding skin for the first 12 months. UV exposure on immature scar tissue causes hyperpigmentation that often becomes permanent, and is the single biggest reason scars look worse than they could.
The protocol is simple. SPF 50+ broad-spectrum applied directly to the scar, every morning and after any wash, for the full first year, indoors and out. A small dedicated tube kept next to your toothbrush gives you the best chance of doing this consistently. After the first year, normal sunscreen use during sun exposure is fine; you no longer need a daily application on the scar specifically.
Patients with multiple atypical moles, mole mapping in progress, or a personal history of skin cancer should treat sunscreen as part of their daily routine rather than a summer or holiday item. Daily SPF 30+ on face, neck, ears and the back of the hands, year-round, with SPF 50+ in summer and on holidays, is the standard recommendation across UK dermatology for high-risk patients.
Common questions
Frequently asked
References
Sources cited
- Marionnet C, Tricaud C, Bernerd F. Exposure to non-extreme solar UV daylight: spectral characterization, effects on skin and photoprotection. Int J Mol Sci. 2014;16(1):68-90. View source
- Petersen B, Wulf HC. Application of sunscreen, theory and reality. Photodermatol Photoimmunol Photomed. 2014;30(2-3):96-101. View source
- Diffey BL. When should sunscreen be reapplied? J Am Acad Dermatol. 2001;45(6):882-885. View source
- Public Health England / NHS. Vitamin D and sunlight: government recommendations. 2016 (updated). View source
- British Association of Dermatologists. Sunscreen factsheet and sun awareness materials. View source
- Green AC, Williams GM, Logan V, Strutton GM. Reduced melanoma after regular sunscreen use: randomized trial follow-up. J Clin Oncol. 2011;29(3):257-263. View source