



Most moles are harmless. Across an adult lifetime the average person carries between 10 and 40 of them, and the overwhelming majority will never become anything more concerning than a cosmetic question. But melanoma, the deadliest form of skin cancer, almost always announces itself first by changing the appearance of a single mole, and that change can be subtle.
The ABCDE framework is the simplest reliable way for a non-specialist to notice the early signs. It was designed in 1985 by a team at New York University[1] and has since been refined and validated in study after study. It is not diagnostic, no patient-administered checklist can be, and only a GMC-registered consultant with dermatoscopy can confirm what a mole actually is. But it is the closest thing the public has to a screening tool, and it works.
This guide walks through each letter, what it actually means in practice, where it falls short, and the additional patterns dermatologists use alongside it. By the end you should be able to look at the moles on your own body with sharper eyes, and know with confidence when something deserves a GMC-registered consultant's attention.
What ABCDE actually is
The ABCDE framework is a five-letter mnemonic that captures the visual features most strongly associated with melanoma. It was developed at New York University in the mid-1980s as a public-education tool, designed specifically to be memorable enough to use without medical training and rigorous enough to flag the right lesions for clinical follow-up. The original four-letter version, ABCD, was extended to ABCDE in 2004 to capture the importance of change over time.[2]
It is the framework every GMC-registered consultant dermatologist will use during a mole check, and it is the same framework taught to medical students and GPs across the UK. Polarised dermatoscopy, the magnification technique used during a clinical assessment, layers far more nuance on top of ABCDE,[3] including pigment networks, vascular patterns and structural symmetry that are invisible to the naked eye, but the mnemonic remains the entry point.
What ABCDE is not, importantly, is a diagnosis. A mole that scores poorly on one or even two letters is not necessarily melanoma. Many entirely benign moles are mildly asymmetric, have a soft colour gradient, or sit just above 6mm. The skill lies in pattern recognition across all five features, which is exactly what an expert eye plus dermatoscopy is for. Use ABCDE as a screening tool, not a verdict.
A, Asymmetry
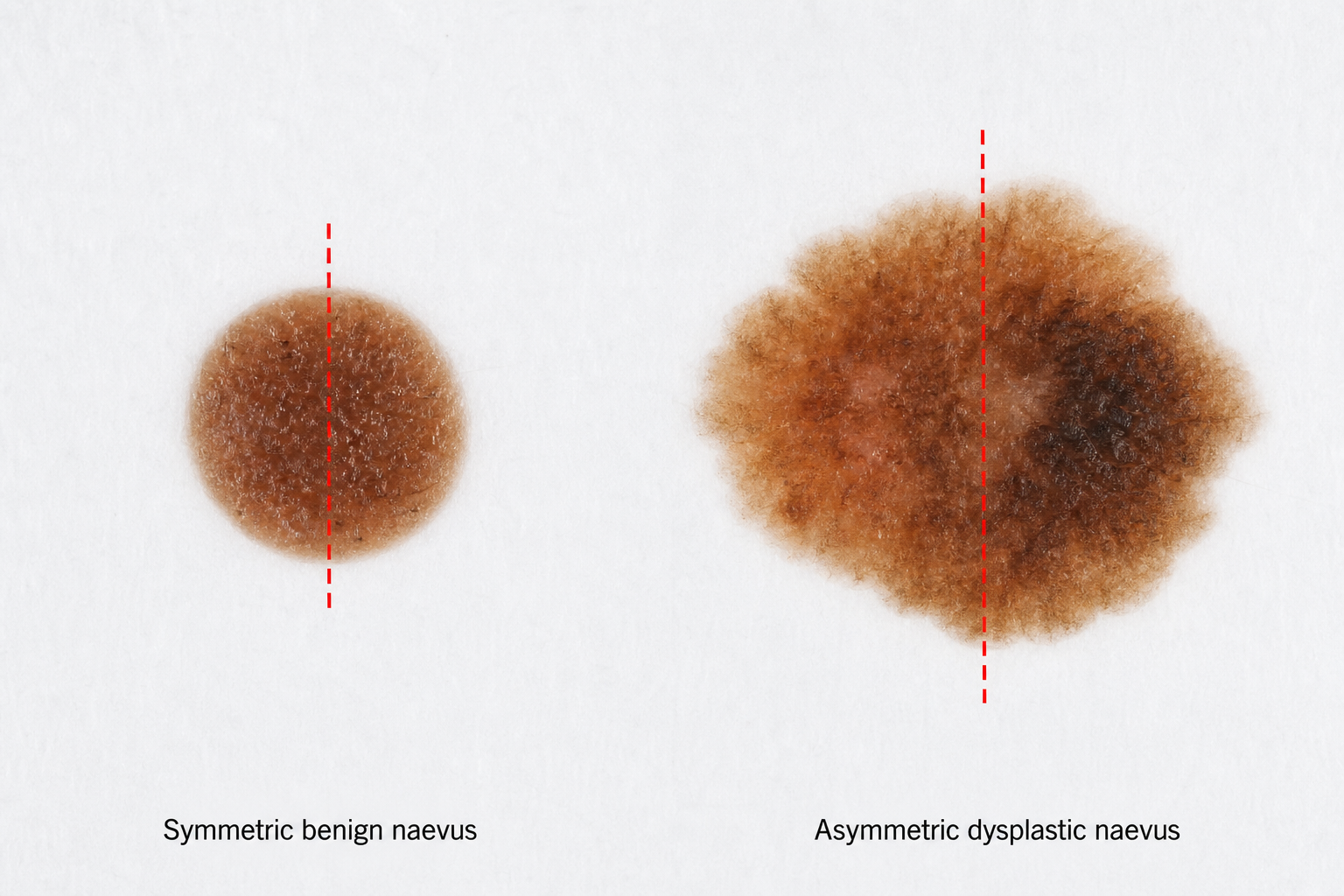
Imagine drawing a line through the centre of the mole, in any direction. If the two halves match, in shape, in colour and in pattern, the mole is symmetrical. If they don't, it is asymmetric, and that is the first feature on the ABCDE list because it is the most consistent visual difference between benign moles and melanomas.
Benign moles typically grow outward from a single melanocyte cluster, which produces a roughly round or oval shape with the same pattern on each side. Melanoma cells, by contrast, grow chaotically. The cells multiply at different rates in different directions, which produces a lesion that looks lopsided, with one half larger or differently coloured than the other.
Mild asymmetry, on its own, is not enough to act on. Plenty of benign moles are slightly oval or slightly irregular. What dermatologists look for is asymmetry that is striking when held up against the rest of your moles, particularly asymmetry that has appeared or worsened over time. If you are checking your own skin, the simplest test is a phone-camera comparison: photograph the mole, then mentally fold the image in half along its longest axis and see if the two halves overlap.
B, Border
A benign mole has a clean, well-defined edge. The pigmented area stops cleanly against the surrounding skin, and the boundary, although not always perfectly smooth, is consistent in colour and clarity all the way around the lesion.
Melanoma borders behave differently. The most common pattern is a notched or scalloped edge, where the boundary moves in and out as if a small bite has been taken from the lesion. Less commonly, the edge can fade gradually into surrounding skin, with no clear stopping point at all. This faded border, sometimes called pigment regression, can be a warning sign even when the rest of the mole looks unremarkable.
Two practical points. First, under a phone macro lens or a high-magnification mirror, almost every mole looks slightly irregular at the edges. The relevant question is not whether the border is geometrically perfect, it is whether the border is consistent with itself. A mole with a clean rounded edge on three sides and a notched, fading edge on the fourth is the kind of asymmetry that warrants a check. Second, borders evolve. A mole whose edges used to be sharp and now appear blurred, even subtly, is a mole worth showing a consultant.
C, Colour
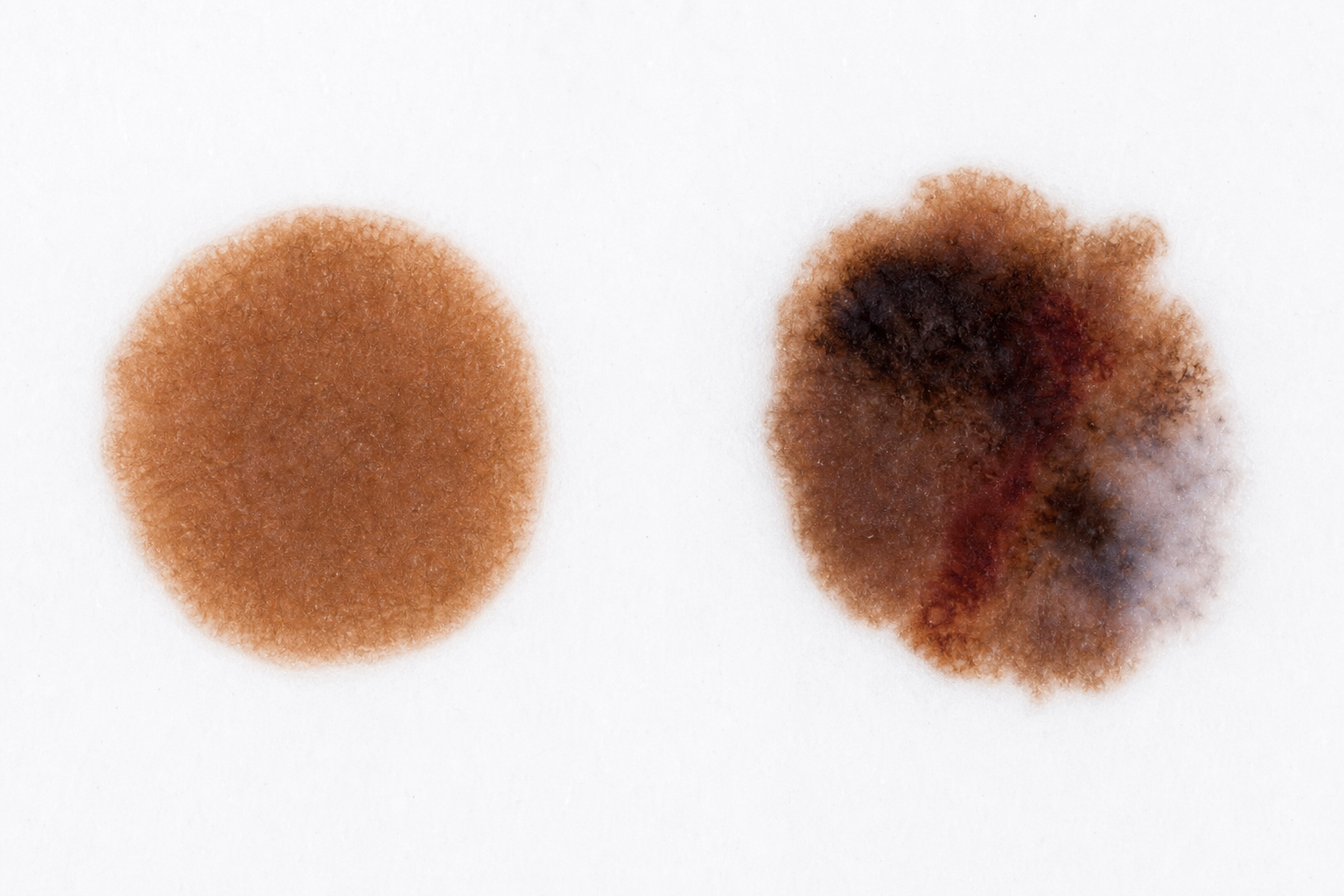
A benign mole is usually a single shade of brown. The shade can be light or dark, the texture can vary, but the colour itself is largely uniform across the lesion. Some patients have moles that are pink or skin-coloured, particularly intradermal moles, and the same standard applies, one colour, applied evenly.
Multiple colours within a single mole is one of the strongest individual ABCDE features. Patches of black against a brown background, areas that have become red, blue, white or grey, or any sense of multiple shades layered on top of each other, all warrant a consultant's eye. The presence of black or blue-grey pigment in particular is associated with deeper melanocytic activity, which can correspond to deeper invasion of the skin.
White or hypopigmented patches inside an otherwise pigmented mole are worth singling out. They can indicate regression, which is the body's immune system attacking a portion of the lesion. Regression sometimes appears in benign moles, but it can also be a marker of melanomas that have started to elicit an immune response, and it deserves a closer look either way.
D, Diameter
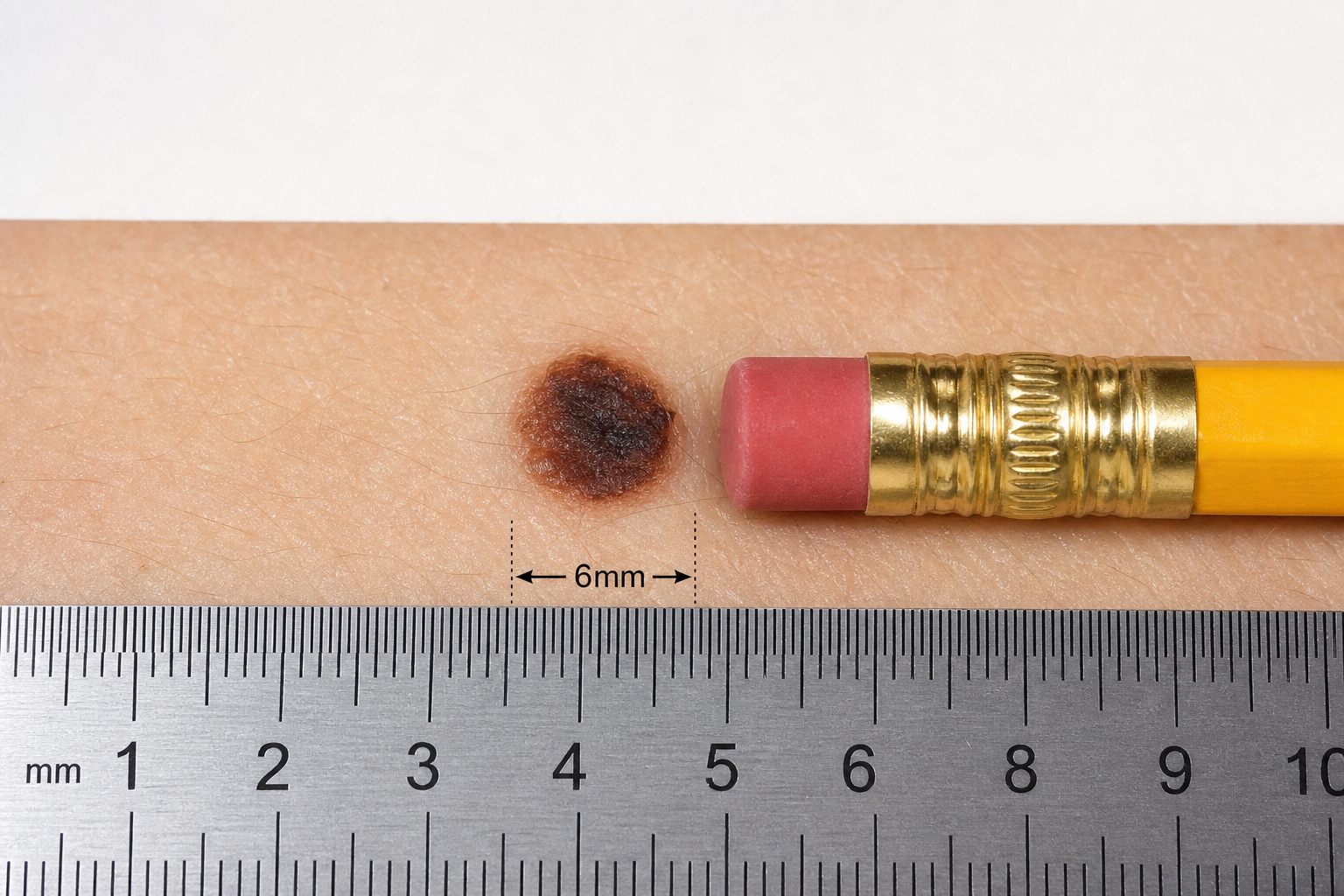
The classical ABCDE rule is that any mole larger than 6mm in diameter, roughly the size of a pencil eraser or the back of a standard biro, deserves attention. The 6mm threshold is not a hard cut-off but a reasonable trigger: most early melanomas, by the time they become clinically obvious, have crossed it.
The reverse rule does not hold. A mole smaller than 6mm is not automatically safe. Early-stage melanomas can be 3 or 4mm across at the time of detection, particularly if they are caught in the very earliest superficial spreading phase. Diameter is best used as a filter, not a guarantee. Anything above 6mm warrants a check, and anything that has grown in size warrants a check regardless of where it currently sits on the ruler.
For self-checking, comparison is more useful than measurement. The size of any individual mole matters less than how it compares to your other moles, and how it compares to itself a year ago. A new 4mm mole appearing in adulthood, in someone whose other moles are smaller, is more interesting clinically than an established 8mm mole that has been the same size for thirty years.
E, Evolving
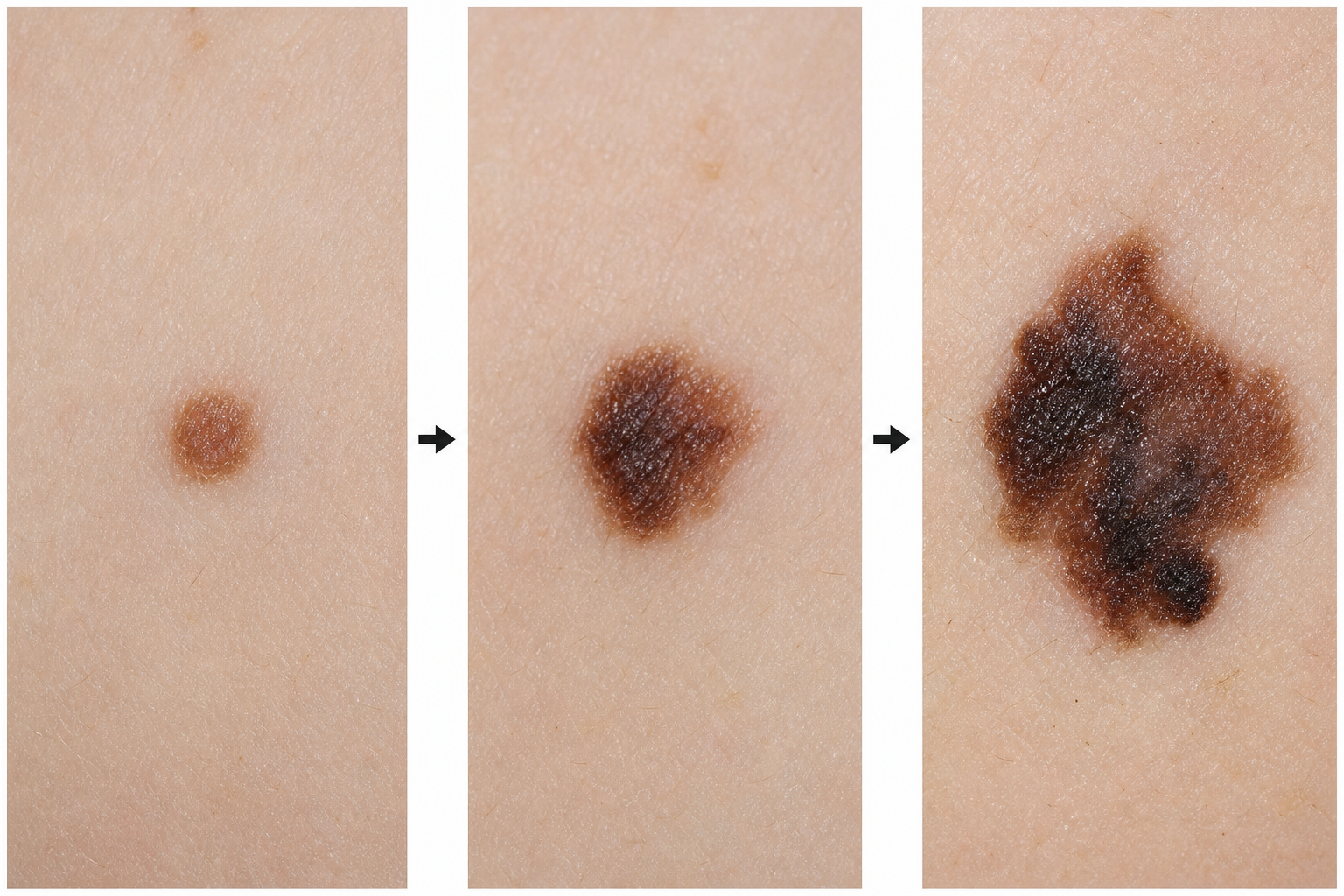
If only one ABCDE feature could be tracked, it would be this one. Change over time is the single most important variable in melanoma detection, and it is the feature that catches early lesions long before any of the static features (asymmetry, border, colour, diameter) become obvious.
Change can take many forms. Growing is the most familiar, but evolution also covers raising, where a previously flat mole begins to lift off the skin; darkening or lightening, where the colour shifts noticeably; and the appearance of new symptoms, itching, bleeding, oozing or crusting, that were not there before. Any of these changes, observed over weeks or months, is sufficient grounds to book a check, even if the mole itself does not yet look dramatically abnormal.
The practical difficulty is memory. Most patients cannot reliably recall what a specific mole looked like a year ago, which is exactly the gap that mole mapping fills. For high-risk patients, with a personal or family history of melanoma, more than 50 moles, or significant sun exposure, photographic comparison at annual intervals is the strongest tool available for catching change at its earliest, most treatable stage. Even without formal mapping, a phone photograph of any mole you find interesting, dated and stored, is worth more than the mental impression you will have a year from now.
Beyond ABCDE: the ugly duckling sign
ABCDE is a checklist applied to one mole at a time. The ugly duckling sign is the complementary observation that comes from looking at the whole canvas. The principle: most people's benign moles share a family resemblance. They tend to look like each other, in shape, in shade and in size. The mole that does not, the ugly duckling, is the one to investigate, even if it does not score badly on any individual ABCDE letter.
The ugly duckling sign is particularly useful for patients with many moles. If you have 30 or 40 lesions across your back and chest, working through ABCDE on each one is impractical. But scanning the whole field for the lesion that looks different from its neighbours is fast, intuitive and well-validated as a screening method.[4]
A related framework, EFG, captures three additional features that matter specifically for nodular melanoma,[5] a less common but more aggressive subtype. Elevated, the lesion is raised rather than flat. Firm, it feels harder than the surrounding skin. Growing, it has visibly changed size in the past month or so. Nodular melanomas can develop quickly and do not always show classical ABCDE features, so EFG is worth knowing about alongside the main framework.
Where ABCDE falls short
ABCDE is a screening tool, not a diagnostic one, and it has known blind spots. Three are worth flagging.
First, amelanotic melanomas, melanomas that produce little or no pigment, can fail every colour-based ABCDE feature. They appear pink, red or skin-coloured, often without the asymmetry or border irregularity that pigmented melanomas display. They are uncommon, around 5% of melanoma cases,[6] but they are routinely missed by self-checking because they do not fit the visual profile. Any new pink or skin-coloured lesion that grows or persists deserves a consultant's eye.
Second, nodular melanomas can develop rapidly and present as raised, dome-shaped lesions that may not show the asymmetry, border irregularity or multi-tone colour of superficial spreading melanomas. EFG is the better framework for nodular detection.
Third, hidden sites are routinely under-checked. Scalp, behind the ears, soles of the feet, under the nails, between the toes, and the back are all areas where melanomas regularly arise and are often missed for months because the patient cannot easily see them. A partner's eye, or a clinical examination, is far more reliable for these areas than self-inspection.
When to act, when to wait
A practical rule of thumb. If a mole shows any single ABCDE feature strongly, book a check. If it shows two or more, even mildly, book a check. If you are unsure, book a check. The cost of an unnecessary appointment is one consultation; the cost of waiting too long with a real melanoma is incomparably higher.
There is no point waiting to see if a mole settles. Benign moles do not begin asymmetric and become symmetrical, and do not begin multi-toned and become uniform. Once a mole is showing change, the change does not reverse. The only useful question is how quickly you can get a consultant's opinion.
The waiting-list framing that applies to many NHS pathways does not apply here. We see suspect-mole patients within five working days, perform consultant-level dermatoscopy in the same visit, and where indicated arrange same-day full-thickness excision with histology. You should leave the appointment with answers, not a referral letter. Most patients who book a Skin Cancer Check receive complete reassurance the same day. The minority who need treatment are usually seen, treated and reported on inside two weeks of first contact.
What actually happens at a mole check
A standard mole check is a 30-minute appointment with a GMC-registered consultant dermatologist. It begins with a brief history, sun exposure, family history of skin cancer, anything you have noticed changing. Each lesion you have flagged is examined visually, then with a high-magnification polarised dermatoscope. If clinically appropriate, the surrounding skin is also given a structured visual scan, and any other lesion of concern is added to the assessment.
Findings are walked through in plain language at the end. Most patients receive complete reassurance: the lesions are benign, no further action is needed beyond ongoing self-monitoring. If a lesion is borderline, the appropriate next step is usually photographic monitoring at 3 to 6 months, not immediate excision. If a lesion is dermatoscopically suspicious, full-thickness excision with histology can be performed in the same visit, no separate appointment, no waiting list, no referral to navigate.
A written report is issued within 24 hours and, with your consent, copied to your GP for their records. The £250 fee is fixed and self-pay only, no insurance pre-authorisation, no excess, no surprise bills. We accept card, Apple Pay, Google Pay and bank transfer.
The framework you have just read is what your consultant will use during the appointment, with the addition of dermatoscopic detail invisible to the naked eye. You should be able to follow the reasoning every step of the way, and ask questions in plain English. That is the standard our consultants are trained to.
Common questions
Frequently asked
References
Sources cited
- Friedman RJ, Rigel DS, Kopf AW. Early detection of malignant melanoma: the role of physician examination and self-examination of the skin. CA Cancer J Clin. 1985;35(3):130-151. View source
- Abbasi NR, Shaw HM, Rigel DS, et al. Early diagnosis of cutaneous melanoma: revisiting the ABCD criteria. JAMA. 2004;292(22):2771-2776. View source
- Vestergaard ME, Macaskill P, Holt PE, Menzies SW. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting. Br J Dermatol. 2008;159(3):669-676. View source
- Grob JJ, Bonerandi JJ. The 'ugly duckling' sign: identification of the common characteristics of nevi in an individual as a basis for melanoma screening. Arch Dermatol. 1998;134(1):103-104. View source
- Kelly JW, Chamberlain AJ, Staples MP, McAvoy B. Nodular melanoma: no longer as simple as ABC. Aust Fam Physician. 2003;32(9):706-709.
- McClain SE, Mayo KB, Shada AL, Smolkin ME, Patterson JW, Slingluff CL Jr. Amelanotic melanomas presenting as red skin lesions: a diagnostic challenge with potentially lethal consequences. Int J Dermatol. 2012;51(4):420-426. View source


